
Pathology of the lacrimal ducts
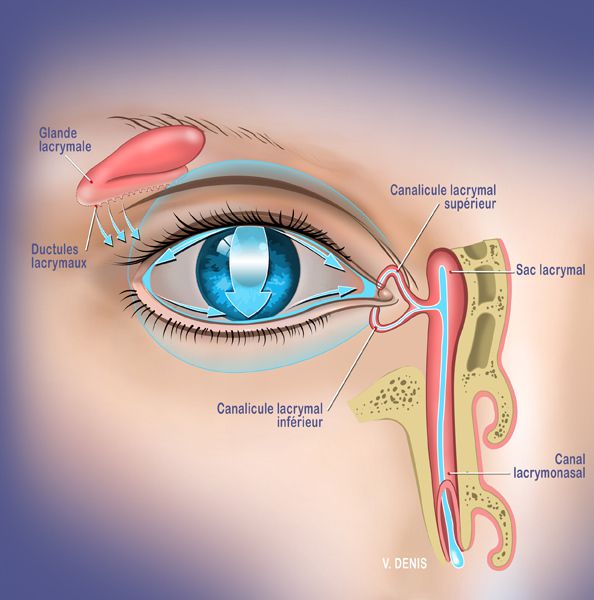
The tear ducts are part of the lacrimal system responsible for the secretion of tears, the circulation of tears, as well as the evacuation of tears from the eyes to the nose.
Pathologies of the tear ducts can lead to tearing linked to:
- excessive production of tears by the main lacrimal gland,
- a defect in the circulation of tears in the eye along the eyelid,
- a tear quality problem
- an obstruction in the evacuation pathways of the tear duct
Pathologies affecting the main lacrimal gland are often inflammatory, infectious or infiltrative diseases. Having little impact on tearing, they are considered diseases of the orbit rather than the tear ducts.
On the other hand, certain medications increase the basal secretion of the main lacrimal gland.
Likewise, there may be hypersecretion of reflex tears by the lacrimal gland in reaction to local irritation (blepharitis, trichial eyelash, foreign body, malposition of the eyelids).
Pathologies concerning the circulation of tears are linked to a problem of eyelid statics. In fact, normally each blink of the eyelid allows tears to pass from the lacrimal gland to the tear duct through the eyelids. When blinking does not occur correctly due to relaxation of the muscle of the ligaments and the tarsus of the eyelid, there is an accumulation of tears at the free edge of the eye causing tearing.
Tear drainage pathologies are essentially secondary to mechanical obstruction of the lacrimal ducts. There may be a stenosis in the lacrimal meatus, the canaliculus, the lacrimal sac or the lacrimonasal duct. Tears then accumulate in the eyelid or lacrimal sac, causing daily and permanent watering of the eyes.
Dr Bela, a specialist in ophthalmology and oculoplasty, treats all lacrimal duct pathologies in her practice.
Treatment of watery eyes
The treatment of tearing eyes depends on the pathologies causing the tearing.
When it comes to excessive tear production it is necessary to look for the cause such as taking medication that increases tear production, the presence of reflex tearing secondary to evaporative dryness on a inflammatory eyelid pathology called blepharitis.
It may be reflex tearing due to an irritating factor such as a poorly positioned eyelash rubbing on the eye, a foreign body located on the cornea or in the eyelid, allergic or infectious conjunctivitis.
When it comes to a lack of evacuation of tears it is necessary to look for stenosis in the path of the tear ducts. This is done in consultation using a probe placed in the tear duct which allows rinsing of the tear ducts. Depending on the behavior of the tears secondarily to this probing, it is possible to evaluate where the stenosis of the tear ducts is located.
When stenosis is suspected, your ophthalmologist will prescribe an additional examination: a dacryoscanner, in order to assess the precise location of this obstruction responsible for the tearing.
Treatment of watery eyes in children
Most often in children it is mechanical tearing linked to congenital stenosis in the lacrimal ducts.
These pathologies are linked to an imperforation of the valve located distally at the level of the tear duct, close to the nasal cavity. This is more common in premature babies.
Obstruction of the tear ducts results in clear, chronic and permanent tearing, from birth. It is unilateral or bilateral. This tearing is often worrying for parents but not very disabling in the development of the child’s vision. It can, however, cause repeated conjunctivitis due to the stagnation of tears in the lacrimal sac.
Additional examinations
In the office we carry out a complete slit lamp examination of the eyes and the appendages of the eye: lacrimal gland, eyelids, tear duct, to look for the causes of the tearing. We do not do x-rays or scans on children.
Treatment
From birth to the fourth month 98% of children recover spontaneously. The tear duct perforates spontaneously, aided by the growth of the child or with the help of daily massage of the tear sac without further treatment.
When the problem persists despite everything, it is necessary to carry out an operation in the operating room under a short general anesthesia.
- Between the fourth and the twelfth month we can offer a simple catheterization in the operating room in the event of frequent secondary infections.
- From 1 year of age catheterization associated with intubation using a silicone probe is indicated. There are no incisions, everything is done naturally. The procedure is performed on an outpatient basis under general anesthesia. The probe is left in place for 6 to 8 weeks then is removed in the office without anesthesia and without pain.
- From 6 years of age in the event of failure of previous treatments, tear duct diversion surgery is offered, in the operating room under general anesthesia. A probe is then put in place for 3 months and removed in the office without anesthesia and without pain.
Treatment of watery eyes in adults
- In adults, tearing is most often secondary to reflex hypersecretion or evaporative hypersecretion due to blepharitis. The tearing is then bilateral and fluctuating: it predominates in wind and cold.
- When it comes to a problem of sagging of the eyelids, the tearing is unilateral or bilateral. The edge of the eyelid is poorly positioned: either rolled inwards against the eyeball, it then rubs the cornea. Either everted outwards, the edge then appears red and irritated and far from the eyeball. The eyes are constantly running and the eye appears red and irritated.
- When tearing is linked toobstruction of the tear ducts, the tearing is unilateral or bilateral. The eyes are constantly running. The tears are clear or purulent depending on the location of the obstruction.
Additional examinations
- A complete eye examination will be carried out in consultation by your Geneva ophthalmologist in order to eliminate an irritating cause: blepharitis, malposition of the eyelids, trichiatic eyelash or foreign body.
- Then a probing and rinsing of the lacrimal ducts will be carried out with physiological serum by your ophthalmologist, Doctor Bela, to determine the degree of stenosis and prescribe the necessary additional examinations. This is done in the office, without anesthesia and without pain.
- A dacryoscanner is often prescribed to identify the location and degree of obstruction and explore the surrounding ENT cavities
Treatment
Treatment varies depending on the cause of the tearing:
- In the event of hypersecretion, the inflammation of the eyelids must be treated and the foreign body or poorly positioned eyelash must be removed
- In the event of tearing due to malposition of the eyelids, surgery to re-tension the eyelids should be considered (see Eyelid pathologies: Entropion / Ectropion)
- In case of obstruction, treatment depends on the degree of stenosis along the path of the tear ducts. The proposed treatment will be surgery to unblock the lacrimal sac directly into the nasal cavity.
> partial stenosis: intubation of the lacrimal ducts using a silicone probe under general anesthesia, on an outpatient basis.
> complete stenosis: lacrimal duct diversion surgery: DCR or Dacryocystorhinostomy. This is a surgical procedure which creates a new flow path for the lacrimal ducts . The flow will still be in the nose but via another route. A probe is placed at the end of the intervention in this new route. This surgery is performed in the operating room externally by directly approaching the lacrimal sac or endonasally assisted by an ENT aided by a camera in the nasal cavity.
1 hour with an overnight stay
general
- Anesthesia consultation before surgery
- Be fasting on the day of the operation
- Exit the next day without dressing
- A probe is placed, visible in the inner corner of the eye but without pain
- Do not blow your nose, do not rub your eye or pull on the probe
- Tearing persists until the probe is removed
Day 1: Appointment with Dr Bela to remove the dressing
Day 7: removal of sutures
M1: final result
How do you treat watery eyes?
Excessive tearing, also known as epiphora, is most often linked to problems with the ocular surface. You should avoid irritants such as cigarette smoke, rinse your eyes with saline solution, use moisturising eye drops and consult your ophthalmologist in Geneva as soon as possible. Your ophthalmologist will carry out a complete eye examination to determine the cause of your watery eyes.
Why do some eyes always cry?
Some eyes may weep chronically as a result of conditions that cause reflex tearing. These include inflammatory conditions of the eyelids, such as blepharitis, or of the conjunctiva, such as allergic or infectious conjunctivitis, or traumatic conditions, such as the presence of a foreign body on the eyelids or cornea, or a poorly positioned eyelash rubbing against the eye. The other main diagnostic framework for chronic lacrimation is that of an obstruction to the evacuation of tears along the lacrimal pathway. This must be determined by a full examination of your eyes in the office of your ophthalmologist in Geneva.
Why do my eyes burn and weep?
In general, the symptoms of burning eyes are associated with reflex tearing. This burning is often linked to a problem of dry eyes. When the eyes no longer produce enough tears, or when these tears evaporate too quickly, there is a reflex in the eyes causing eye burning and reflex tearing associated with excessive blinking. Ocular fatigue can also lead to dry eyes after prolonged exposure to screens. It can also involve the presence of toxic tears causing reflex tearing, as in the case of allergic conjunctivitis, exposure to toxic smoke or chemical splashes in the eyes.
How can you tell if your tear duct is blocked?
Only your ophthalmologist will be able to assess whether your tear duct is blocked. During a consultation, they will carry out a complete examination of your eye to assess the quality of your tears, the presence of a foreign body in the eyes or eyelids, or a stenosis in the lacrimal duct or lacrimal sac. This examination will be completed by a lacrimal duct catheterisation to confirm the diagnosis of lacrimal duct obstruction.
What is lacrimal duct obstruction?
The lacrimal ducts extend from the orifice inside the eyelids into the nasal cavity. The lacrimal ducts are divided into different sections, from the lacrimal meatus, to the canaliculus, the lacrimal sac and the lacrimonasal duct. Obstructive pathologies can occur along this entire pathway, making it impossible to evacuate tears and causing one or both eyes to water daily. This obstruction is most often mechanical and has no known cause, but it may be secondary to the presence of post-inflammatory fibrosis, ENT surgery, chronic inflammatory disease of the sinuses, or a tumour in the lacrimal duct. In all cases, obstruction of the tear ducts causes watering.